

Australian guidance on clean and safe environments is clear on the core expectation: providers need processes that maintain a clean, safe and hygienic environment, respond to environmental risks, use appropriate cleaning and disinfection products, train staff for routine and outbreak cleaning, and monitor whether cleaning is effective. The Australian Commission on Safety and Quality in Health Care also frames environmental cleaning as part of infection prevention, with documented schedules, staff training, risk response and routine evaluation all treated as evidence of a controlled system.For aged care providers, this connects directly to Aged Care Quality Standards expectations around a safe service environment, infection prevention and clinical governance. The standard is not simply “the facility looks clean”. A facility should be able to show that its environmental cleaning system is deliberate, risk-assessed and consistently implemented.
How to achieve the Environmental Cleaning Standards
In practical terms, an aged care environmental cleaning standard should cover:
- A documented cleaning schedule for every area of the facility
- Clear cleaning frequencies based on infection risk, resident vulnerability, surface type, touch frequency and whether the area is shared.
- Products that are suitable for healthcare or aged care use, including Therapeutic Goods Administration (TGA) or Australian Register of Therapeutic Goods (ARTG) listed disinfectants, where required.
- Instructions for product dilution, contact time, compatibility with surfaces, safe storage and expiry.
- Defined roles for cleaners, care workers, nurses, maintenance teams and external contractors.
- Staff training in infection control procedure, PPE, hand hygiene, spill response, waste handling and equipment management.
- Evidence that cleaning has occurred, such as signed schedules, supervisor checks, spot audits, corrective actions and training records.
The important point for managers is that standards are judged through systems and evidence. If a resident bathroom is cleaned every morning but there is no risk-based schedule, no method, no product record and no audit trail, the facility is exposed. If cleaning frequency is increased during an outbreak but the escalation trigger is not documented, it becomes difficult to prove that the response was controlled.
Building A Risk-Based Environmental Cleaning Schedule
A good cleaning schedule starts by dividing the facility into risk areas, then assigning the right method and frequency to each area. These include:
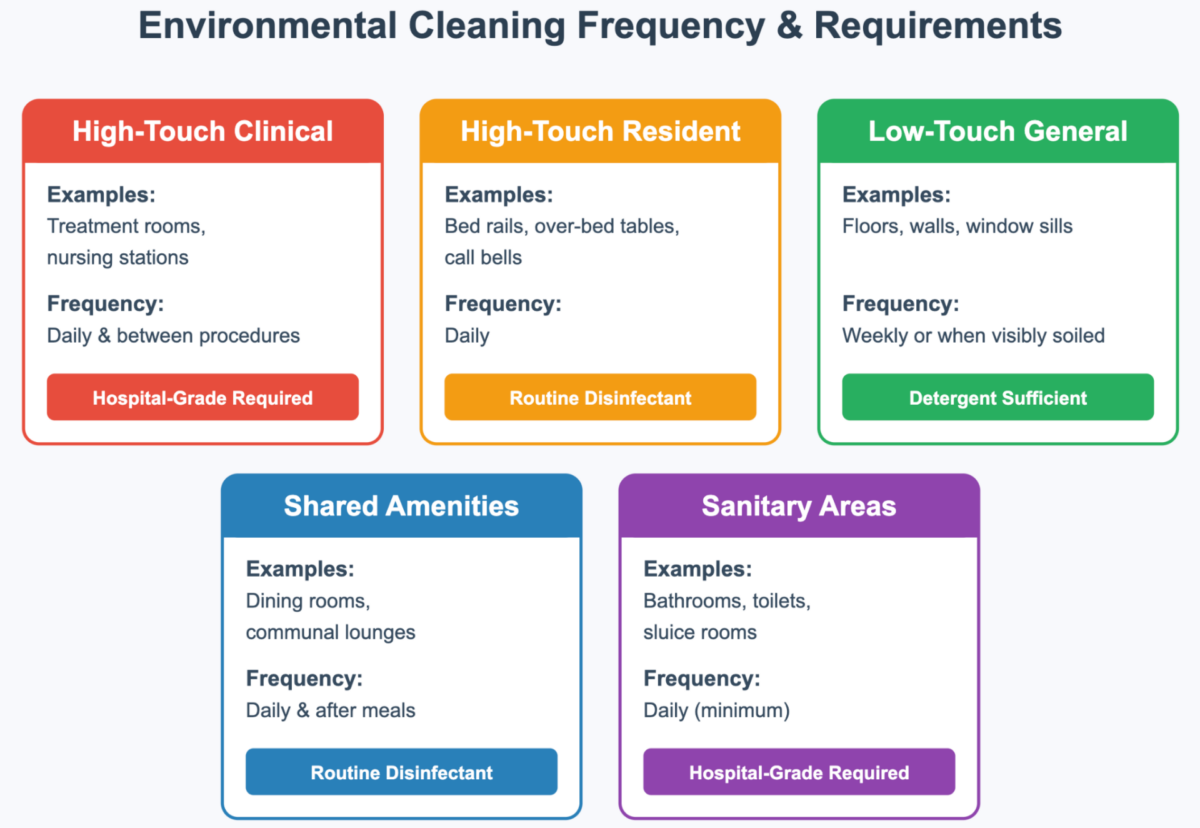
High-Touch Clinical Areas
High-touch clinical areas include treatment rooms, medication preparation areas, nursing stations, clinical benches, shared clinical equipment and spaces where wound care, observations or other procedures occur. These areas need stronger controls because they sit close to direct care and clinical decision-making.
Cleaning should be scheduled at least daily, between procedures where relevant, and immediately when contamination is visible. Surfaces should generally be cleaned and disinfected using a hospital-grade product, with attention to contact time. Benches, keyboards, workstations on wheels, blood pressure cuffs, thermometers and shared devices should not be missed simply because they are not part of the floor or furniture schedule.
The procedure should also define what happens before and after a clinical task. For example, a treatment trolley should be cleaned before restocking, after use and before being moved back into a clean storage area. If the trolley moves between rooms, the cleaning process becomes part of cross-contamination control.
High-Touch Resident Areas
Resident rooms are personal spaces, but they are also care environments. Bed rails, over-bed tables, call bells, chair arms, mobility aids, remote controls, light switches, door handles and bathroom grab rails are touched repeatedly throughout the day. These surfaces should be cleaned and disinfected at least daily, with more frequent cleaning when a resident has respiratory symptoms, diarrhoea, vomiting, a wound infection or increased personal care needs.
The cleaning method must protect dignity as well as hygiene. Staff should explain when cleaning is happening, avoid moving personal items unnecessarily, and use a consistent sequence so surfaces are not missed. A common method is to work from cleaner areas to dirtier areas, from high surfaces to low surfaces, and from the resident zone towards the exit.
This is also where environmental cleaning overlaps with care staff practice. If a call bell falls onto the floor or a walking frame is visibly soiled, waiting for the next scheduled clean is not enough. The process should tell staff when to spot clean, when to notify cleaning staff, and when an item needs to be removed from use until cleaned.
Low-Touch General Areas
Low-touch surfaces include walls, window sills, ceilings, vents, skirting boards and some floor areas. These usually require less frequent cleaning than high-touch surfaces, but they still belong in the environmental cleaning programme. Dust, moisture damage, mould, poor ventilation, clutter and damaged surfaces can all increase infection or safety risks.
For low-touch areas, detergent cleaning may be sufficient during routine cleaning unless there is visible contamination, outbreak guidance or a specific risk. The schedule should still nominate frequency, method and responsibility. “As needed” is too loose unless it is supported by inspection criteria.
Maintenance matters here. Cracked vinyl, damaged furniture, peeling paint and worn seals can make proper cleaning difficult. Environmental cleaning standards are therefore linked to the condition of the building, fixtures and fittings. If a surface cannot be effectively cleaned, it should be repaired, replaced or risk assessed.
Shared Amenities
Dining rooms, lounges, activity rooms, reception areas, corridors and shared seating are high-risk because many people use them in short periods. These spaces are where a visually tidy facility can still fall short of environmental cleaning standards.
Dining tables and chair arms should be cleaned and disinfected after meals. Handrails, door handles, lift buttons, shared remotes, activity tables and communal touch points should be cleaned at least daily, and more often during respiratory virus season or when illness is present in the facility. Shared equipment, including games, tablets, mobility aids and therapy equipment, needs a clear clean-after-use rule.
The schedule should also account for timing. Cleaning a dining room before lunch is useful, but it does not address contamination left after meals. Cleaning a lounge once in the morning may not be enough if visitors, residents and staff use the same touch points all afternoon.
Sanitary Areas
Bathrooms, toilets, en-suites, sluice rooms, pan rooms and soiled utility areas require the strictest separation of clean and dirty workflows. These areas are more likely to involve body fluids, contaminated linen, continence products, waste and high-touch fixtures.
At a minimum, sanitary areas should be cleaned and disinfected daily, with spot cleaning whenever contamination occurs. Toilets, flush buttons, taps, basins, grab rails, shower chairs, commodes, door handles, and floors around fixtures need explicit inclusion in the schedule. In shared bathrooms, cleaning frequency should reflect actual use rather than a generic daily routine.
Sluice rooms and soiled utility areas should have their own procedures for waste movement, PPE, cleaning equipment, hand hygiene and storage. Clean supplies should not be stored beside soiled items, and cleaning tools used in sanitary areas should be colour-coded or otherwise separated from tools used in kitchens, dining areas or resident rooms.
Real-Life Example: Gastro In A Shared Dining Room
Consider a resident who vomits in a shared dining room shortly after lunch. If the response is treated as general tidying, staff may remove the visible mess, wipe the table quickly and reopen the room. That does not meet the standard of environmental cleaning because the risk is not limited to the visible spill.
A proper environmental cleaning response would start by restricting access to the affected area and applying the facility’s body-fluid spill procedure. Staff would put on the required PPE, remove the spill safely, clean the area with detergent, then disinfect the table, chair, floor area and nearby high-touch surfaces using the approved product and contact time. Waste would be disposed of according to the facility’s procedure, and reusable cleaning equipment would be cleaned and disinfected or removed for laundering.
The response should then widen beyond the immediate spill. Because gastroenteritis can spread quickly in aged care, the facility may increase cleaning frequency for dining tables, chair arms, handrails, toilet areas, door handles, lift buttons and shared lounge touch points. The resident’s room and ensuite may require enhanced cleaning and shared equipment used by the resident should be cleaned before reuse, and the cleaning schedule should record the escalation.
This example shows how environmental cleaning connects the standards together: risk assessment, PPE, product selection, correct method, clean and dirty workflows, documentation, staff communication and audit evidence. The facility is not just cleaning a mess. It is controlling an infection risk in a shared care environment.
Training, Auditing, and Evidence For Compliance
Environmental cleaning is only reliable when staff are trained and the work is checked. Training should cover the difference between cleaning and disinfection, high-touch surface priorities, colour-coded equipment, PPE, hand hygiene, chemical dilution, contact time, spill response, outbreak cleaning, waste handling and what to do when a surface or item cannot be cleaned safely.
Auditing should include more than visual inspection. A surface can pass a visual check and still have been cleaned incorrectly. Facilities may use supervisor observation, fluorescent marker testing, ATP testing, cleaning log reviews, product checks, trolley checks and targeted audits after outbreaks or incidents. Namoli Healthcare can help reduce that administrative burden by providing healthcare cleaning teams, supervisor checks, app-based reporting, ATP hygiene verification and audit-ready documentation as part of a managed cleaning service.
Useful evidence includes completed cleaning schedules, outbreak cleaning records, training logs, product safety data sheets, disinfectant approvals, audit results, corrective action records, equipment maintenance logs and risk assessments for problem areas. These records help show that cleaning in aged care facilities is not ad hoc, but part of a controlled IPC system. For facility managers and clinical leads, this is often the main advantage of working with a specialist provider: the cleaning, reporting and compliance support sit within one accountable service instead of being spread across busy internal teams.

Bringing Environmental Cleaning Up To Standard
A strong programme should answer five questions without hesitation:
- What needs to be cleaned?
- How often does it need to be cleaned?
- Which method and product should be used?
- Who is responsible for doing it and checking it?
- What evidence proves it happened?
When those answers are specific, documented and followed, environmental cleaning becomes more than a compliance activity. It becomes a daily safeguard for residents, staff and visitors, and a practical way to reduce infection risk while maintaining a comfortable aged care environment.
If your facility needs a cleaner way to manage risk-based schedules, routine cleaning, terminal cleans, ATP verification and audit-ready records, Namoli Healthcare’s aged care cleaning team can build the programme around your site.



Related Posts


