Topic Tags:
Terminal cleaning, conducted after surgical sessions or patient discharge, ensures operating rooms are safe for the next case. Though the CDC (U.S.) provides a framework for terminal cleaning, Australian healthcare standards require adherence to local guidelines and TGA‑approved products. This article adapts CDC principles to the Australian context.
Key takeaways:
- Outsourcing terminal cleaning to a specialist like Namoli Healthcare ensures compliance with Australian regulations and audit readiness.
- Terminal cleaning is a meticulous process involving cleaning and disinfecting every surface and device in the theatre, not just high‑touch points.
- PPE, hospital‑grade disinfectants and structured checklists are critical to protecting cleaners and ensuring thorough decontamination.
1. Preparation and PPE
Before starting, cleaning staff should don appropriate personal protective equipment—gloves, gown or apron, and eye protection. For rooms that housed patients with airborne infections, a P2/N95 respirator is mandatory. Ventilation plays a vital role in reducing airborne pathogens. Assemble fresh cleaning supplies, including detergent solution, disinfectant wipes and mop heads. Remove all single‑use items, waste and soiled linen; place them in designated bags for disposal.
2. Proceeding from Cleaner to Dirtier
A fundamental principle of hospital and operating room cleaning is to always work from cleaner areas to dirtier areas. This prevents transferring dirt, microorganisms, or contaminants to surfaces that have already been sanitised and reduces the risk of cross-contamination.
Practical applications include:
- Low-touch before high-touch: During terminal cleaning, begin with low-touch surfaces (walls, shelves) before moving on to high-touch points (bed rails, door handles, call bells).
- Patient areas before toilets: Clean the patient’s zone or procedure room areas before addressing patient toilets or adjoining bathrooms.
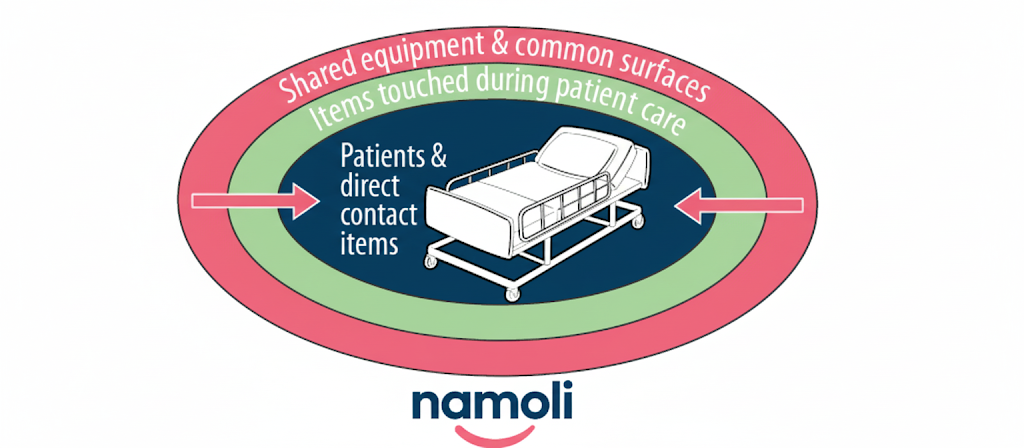
- Inside a patient room: Start with shared equipment and common surfaces, then move to high-touch items outside the patient zone, and finally clean high-touch surfaces inside the patient zone. This order ensures the most frequently contaminated areas are cleaned last, with fresh supplies.
- General areas before isolation areas: Clean open patient care areas not under transmission-based precautions first, before tackling rooms or zones under special precautions, where the risk of contamination is higher.
3. Cleaning From Top to Bottom

A terminal clean begins with a systematic top‑to‑bottom approach. Dust and clean ceiling-mounted lights, tracks and overhead booms. Wipe down walls, window sills and monitors. Clean and disinfect shelves, tables, anaesthesia machines and cables. Pay attention to high‑touch surfaces—door handles, switches, knobs, infusion pumps and control panels—using a TGA‑listed disinfectant. Remove detachable components from equipment, clean them separately and ensure they are dry before reassembly.
4. Decontaminating the Operative Table and Equipment
The surgical table must be meticulously cleaned and disinfected. Remove and discard single‑use covers; wipe the mattress, side rails and attachments with detergent followed by disinfectant, observing the contact time specified by the manufacturer. Clean surgical lights, suction devices, imaging equipment and foot pedals. For reusable instruments that remain in the room, transfer them to the sterile processing department. Ensure sharps containers are replaced if filled beyond the recommended level.
5. Flooring and Low‑Touch Surfaces
After cleaning and disinfecting all equipment and high surfaces, clean the floors. Use a detergent solution for a full mop, working from the farthest corner towards the exit. Change mop heads frequently to avoid spreading contaminants. Once mopped, apply a disinfectant solution if required or use a two step process chemical. Low‑touch surfaces, such as skirting boards, floor drains and storage cupboards, should also be wet wiped down.
6. Final Steps and Documentation
Replace linen, restock supplies and ready the theatre for the next case. Remove PPE in the correct order to avoid contamination (gloves and gown first, then eye protection and mask). Perform hand hygiene immediately after removal. Document the terminal clean with a checklist signed by the cleaner and a supervisor. This record provides evidence of compliance for audits and quality reviews. Check out the CDC Environmental Checklist for Monitoring Terminal Cleaning.

Partnering With Specialist Providers
Given the complexity of terminal cleaning, many hospitals engage specialised providers. Namoli Healthcare offers terminal cleaning services that align with Australian guidelines and adapt CDC frameworks for local standards. Our trained teams use colour‑coded equipment, TGA‑approved disinfectants and thorough checklists to deliver audit‑ready cleaning. We provide documentation and feedback on compliance, helping facilities maintain accreditation and reduce infection risks.



Related Posts
Topic Tags: Sapovirus is a common cause of acute gastroenteritis, particularly in young children and aged‑care settings. Although symptoms are…


Topic Tags: Effective infection control is central to resident safety in aged care, where close living environments, chronic illness, and…
Topic Tags: In healthcare environments, many pathogens spread through high-touch surfaces that look clean but still carry organic residue. Traditional…